Mental Examination Status Examples for Charting

A mental status exam often breaks down not during the assessment itself, but at the point of documentation. The clinician observes useful details, asks the right questions, and still ends up with a note that is vague, inconsistent, or difficult for the next provider to interpret. That is why practical mental examination status examples matter – they help translate clinical observation into language that is specific, defensible, and fast to chart.
The challenge is not finding words. It is choosing wording that is accurate enough to reflect the patient in front of you, standardized enough to support team communication, and flexible enough to fit the setting. An emergency department note should not read exactly like a psychotherapy intake, and neither should mirror an inpatient psychiatric admission without adjustment.
How to use mental examination status examples correctly
Examples are useful when they function as models, not shortcuts. Copying a stock phrase without verifying that it matches the patient creates documentation risk. The better approach is to use examples as structured prompts for what to observe and how to phrase it.
A strong MSE entry does three things. It states what you saw or elicited, avoids unsupported interpretation, and stays internally consistent. If a note says the patient has “normal speech” but later describes “pressured, loud, difficult-to-interrupt verbal output,” the inconsistency weakens the record and can affect handoff decisions.
The safest documentation language is concrete. “Disheveled clothing, poor grooming, limited eye contact” is stronger than “appears depressed.” The former is an observation. The latter may be part of an impression, but it should not replace the descriptive data.
Core mental examination status examples by domain
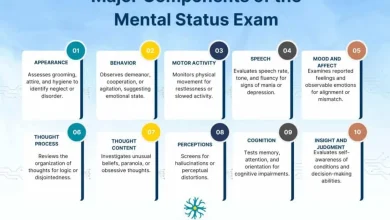
Appearance and behavior
This section should capture visible presentation and observable conduct. Useful phrasing includes: “well-groomed, appropriately dressed for weather, calm, cooperative” or “unkempt, malodorous, wearing layered clothing indoors, intermittently guarded.” For psychomotor activity, examples include “no abnormal movements noted,” “psychomotor agitation with pacing and frequent shifting in seat,” or “psychomotor slowing with delayed initiation of movement.”
Behavioral wording should stay specific. “Suspicious” may be appropriate if the behavior supports it, but “frequently scans room, reluctant to answer, asks repeated questions about confidentiality” gives a clearer clinical picture.
Speech
Speech documentation usually covers rate, volume, quantity, and fluency. Common examples include “speech normal in rate, rhythm, and volume” for a straightforward finding. If abnormal, chart what is abnormal: “speech pressured and loud,” “speech slowed with prolonged latency,” or “minimal spontaneous speech, answers brief but coherent.”
Speech can also help distinguish conditions, but only if the description is precise. “Rambling” is less useful than “verbose, overinclusive responses requiring redirection.” That phrasing tells the next clinician what happened during the interview.
Mood and affect
Mood is generally the patient’s stated emotional experience. Affect is what you observe. This is a section where weak documentation is common. “Mood okay” or “affect normal” rarely adds enough information.
Better examples include: “mood reported as ‘anxious'” paired with “affect constricted but congruent with stated mood.” Other common formulations are “mood ‘depressed,’ affect tearful and restricted,” “mood ‘fine,’ affect irritable and incongruent with stated mood,” or “euthymic mood with full-range, reactive affect.”
The key is not to force technical language when it does not fit. If affect is flat, say flat. If it varies appropriately during the interview, document that. Congruence and range matter when they are clinically relevant, not as routine filler.
Thought process
Thought process describes how ideas are expressed and connected. A normal example is “thought process linear, logical, and goal-directed.” Abnormal examples include “circumstantial thought process with eventual return to point,” “tangential responses with limited ability to return to topic,” or “disorganized thought process with loose associations.”
This section benefits from discipline. Do not document “flight of ideas” unless the patient is actually moving rapidly from topic to topic in a way consistent with that pattern. Under time pressure, clinicians sometimes use high-level labels too loosely. The more serious the descriptor, the more important it is that the note supports it.
Thought content
Thought content addresses what the patient is thinking about, including delusions, obsessions, preoccupations, and suicidal or homicidal ideation. Examples include “denies suicidal ideation, homicidal ideation, and psychotic symptoms,” “preoccupied with somatic concerns,” or “reports persecutory beliefs that neighbors are monitoring his apartment.”
If risk content is present, be exact. “Endorses passive death wish without plan or intent” means something different from “endorses suicidal ideation with plan to overdose.” Documentation should also reflect whether the patient denies, endorses, or cannot adequately answer due to intoxication, agitation, or cognitive impairment.
Perception
This section covers hallucinations and other perceptual disturbances. Standard examples include “no auditory or visual hallucinations reported” or “reports intermittent auditory hallucinations of voices commenting on behavior.” If the patient appears internally preoccupied but does not disclose hallucinations, document the observation separately rather than assuming the symptom.
For example: “frequently pauses as if listening, turns head toward corner of room, denies auditory hallucinations.” That wording preserves clinical nuance without overstating findings.
Cognition
Cognition can be brief or expanded depending on setting. Typical charting examples include “alert and oriented to person, place, time, and situation,” “attention mildly impaired, requires repetition of questions,” or “recent memory grossly intact by interview.” In a more detailed exam, you may document abstraction, concentration, fund of knowledge, or executive functioning.
This is also where setting matters. In an emergency evaluation, a concise cognitive screen may be enough. In neuropsychiatric or geriatric contexts, broad statements like “cognition intact” are often insufficient.
Insight and judgment
These domains are often charted too vaguely. “Poor insight and judgment” is common, but often unsupported. Better examples include “insight limited – does not recognize current symptoms as illness” and “judgment impaired as evidenced by recent high-risk behavior and inability to identify safe discharge plan.” For a stable outpatient, an appropriate note might read: “insight fair, acknowledges anxiety symptoms and need for treatment; judgment intact in routine decision-making.”
The phrase “fair” is acceptable when it reflects a mixed picture, but it should still correspond to observed behavior or reported choices.
Setting-specific charting examples
A useful mental status exam is not one-size-fits-all. The same patient may require different emphasis depending on the workflow and clinical question.
Emergency department
In the ED, the note must support triage, risk assessment, and disposition. Brevity matters, but so does clarity. A practical example is: “Alert, restless, disheveled, speech rapid and loud. Mood ‘panicked.’ Affect anxious and labile. Thought process perseverative on safety concerns. Denies hallucinations. Endorses passive SI without plan or intent. Insight limited, judgment impaired in context of acute distress.”
That level of detail usually serves the setting better than broad labels such as “anxious, stable.”
Inpatient psychiatry
On an inpatient unit, behavioral trends and symptom severity are often more important than polished prose. For example: “Calm and medication adherent on approach, though remains guarded. Speech normal rate, low volume. Affect constricted. Thought process linear. Ongoing persecutory delusions regarding staff intent. Denies current SI/HI. Insight poor. Judgment limited.”
This format gives the team something actionable for treatment planning and daily comparison.
Outpatient behavioral health
Outpatient documentation often benefits from noting baseline function and treatment engagement. Example: “Well-groomed, cooperative, maintains eye contact. Speech normal. Mood ‘stressed,’ affect appropriate and reactive. Thought process goal-directed. No evidence of psychosis. Cognition grossly intact. Insight and judgment good.”
In outpatient settings, normal findings still need enough specificity to show that the exam was actually performed.
Common mistakes when using examples
The biggest mistake is relying on default phrases that flatten the patient presentation. “Within normal limits” may save time, but overuse reduces clinical value. Another frequent issue is mixing objective exam content with diagnostic conclusions. The MSE can support a diagnosis, but it is not the place to substitute labels for observations.
A third problem is failing to update templated language. If yesterday’s note says “denies SI” and today’s encounter involved a suicidal disclosure, imported text can create a serious contradiction. Templates improve efficiency only when they are actively edited.
This is where a standardized framework helps. Resources such as MentalStatusExamTemplate.com are most useful when they reduce omissions without encouraging autopilot documentation.
A practical approach to writing better MSE notes
Start with direct observation, then add patient-reported material, then refine with clinically relevant descriptors. If you are unsure whether a term is warranted, use plainer language. “Easily distracted during interview” is often better than prematurely labeling attention as “impaired” without context.
It also helps to think in pairs: mood with affect, thought process with thought content, insight with judgment. Those pairings reduce gaps and make the note easier to review. Over time, your wording becomes faster because it is organized, not because it is generic.
The best MSE documentation sounds less impressive than many trainees expect. It is concise, specific, and consistent with the rest of the note. If your charting helps the next clinician understand what the patient looked like, how they communicated, what risks were present, and what level of insight they showed, it is doing its job well.
The most useful example is the one that matches the patient accurately enough that another clinician could step in and recognize the same presentation from your note.



One Comment