What Is Included in a Mental Status Exam?

When a chart says “MSE completed,” the value is not in the abbreviation. It is in whether the exam was actually comprehensive enough to support diagnosis, risk assessment, treatment planning, and handoff to the next clinician. That is why understanding what is included in a mental status exam matters far beyond documentation style. A complete MSE gives structure to clinical observation, reduces omissions, and makes your note more useful in fast-moving settings.
What is included in a mental status exam?
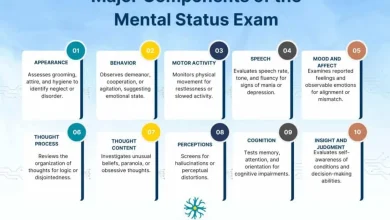
A mental status exam typically includes appearance, behavior, psychomotor activity, attitude, speech, mood, affect, thought process, thought content, perception, cognition, insight, judgment, and an assessment of risk when clinically relevant. In practice, the exact depth of each section depends on setting, presenting problem, and patient capacity to participate.
The key point is that the MSE is not just a checklist of psychiatric symptoms. It is a structured snapshot of current mental functioning based on what you observe, what the patient reports, and how the patient performs during the encounter. In an emergency department, the exam may emphasize orientation, psychosis, intoxication, and immediate safety. In outpatient care, it may place more weight on baseline functioning, cognition, affective range, and insight over time.
Core components of what is included in a mental status exam
Appearance and general presentation
This section documents how the patient presents physically. It usually includes apparent age, grooming, hygiene, dress, nutritional status, eye contact, posture, and any distinguishing features relevant to clinical impression. The goal is not cosmetic description. It is to capture observable details that may support or challenge diagnostic hypotheses.
For example, disheveled appearance, poor hygiene, or inappropriate clothing for weather may suggest psychosis, severe mood disorder, cognitive decline, or functional impairment. At the same time, a well-groomed appearance does not rule out serious pathology. Documentation should stay objective and clinically relevant.
Behavior, attitude, and psychomotor activity
Behavior refers to how the patient acts during the interview. This includes cooperativeness, level of engagement, agitation, guardedness, impulsivity, pacing, retardation, abnormal movements, and response to internal or external stimuli. Attitude often overlaps here and may be described as cooperative, hostile, evasive, suspicious, seductive, or withdrawn.
Psychomotor activity is especially important because it can reflect depression, mania, medication effects, catatonia, intoxication, anxiety, or neurologic issues. A patient who is slowed, staring, and minimally responsive presents a different clinical picture than one who is restless, intrusive, and unable to remain seated.
Speech
Speech is one of the fastest ways to assess mental state, yet it is often documented too vaguely. A useful MSE describes rate, volume, tone, rhythm, spontaneity, articulation, and fluency when relevant. You are looking for abnormalities such as pressured speech, latency, poverty of speech, slurring, mutism, or tangential overproduction.
Speech findings help distinguish between conditions that may otherwise look similar on the surface. A depressed patient may have slowed, quiet speech. A manic patient may have rapid, loud, difficult-to-interrupt speech. A patient with delirium or intoxication may show disorganized or slurred output.
Mood and affect
Mood is the patients subjective emotional state, typically reported in their own words. Affect is your observed impression of emotional expression. A complete MSE addresses both because they are related but not interchangeable.
Mood might be documented as depressed, anxious, irritable, euthymic, overwhelmed, or “fine” if that is the patients stated report. Affect should then describe range, intensity, stability, and congruence with stated mood or discussed content. Terms like constricted, blunted, flat, labile, tearful, bright, or appropriate are more useful than broad labels alone.
The nuance matters. A patient may report feeling “okay” while showing constricted affect and minimal reactivity, or endorse severe depression while laughing inappropriately at distressing content. These discrepancies do not automatically mean malingering. They simply become part of the clinical picture.
Thought process
Thought process describes how ideas are connected and expressed. This is one of the highest-yield parts of the MSE because it helps identify formal thought disorder, cognitive disruption, and severe mood states. Common descriptors include linear, goal-directed, circumstantial, tangential, loose, disorganized, racing, perseverative, or thought blocking.
Clinicians sometimes combine thought process and thought content in a single sentence, but separating them improves clarity. Process is about the form of thinking. Content is about what the patient is thinking about.
Thought content
Thought content includes themes, beliefs, and preoccupations that may have diagnostic or safety significance. This often covers delusions, obsessions, ruminations, ideas of reference, paranoia, guilt, grandiosity, hopelessness, suicidal ideation, homicidal ideation, and violent thoughts.
This section should be specific. “Thought content normal” can miss critical detail and is rarely the strongest documentation choice in acute settings. If there is no evidence of delusions, obsessions, or harmful ideation, say so directly. If these are present, document nature, frequency, intensity, and whether there is intent or plan when relevant.
Perception
Perception addresses hallucinations, illusions, depersonalization, derealization, and response to internal stimuli. Auditory and visual hallucinations are the most commonly documented, but tactile, olfactory, and command hallucinations may be clinically important as well.
Not every unusual sensory experience carries the same weight. Grief-related experiences, trauma phenomena, substance effects, sleep deprivation, and primary psychosis can all affect perception in different ways. The exam should capture what the patient reports and what you observe without prematurely collapsing everything into one diagnosis.
Cognition in the mental status exam
Orientation, attention, memory, and concentration
Cognition is a major part of what is included in a mental status exam, even in settings where the interview is brief. At minimum, most MSEs assess orientation to person, place, time, and situation. Beyond orientation, clinicians often evaluate attention, concentration, immediate recall, recent memory, and remote memory.
The level of detail depends on context. In a psychiatric follow-up, a brief cognitive screen may be enough unless there is concern for neurocognitive disorder, delirium, intoxication, or head injury. In emergency or inpatient settings, cognition may need more focused assessment because it directly affects reliability, capacity, and safety planning.
Fund of knowledge and abstract reasoning
Some exams also include fund of knowledge, estimated intellectual functioning, and abstraction. These elements are more common when cognitive or developmental concerns are relevant, or when a fuller psychiatric evaluation is being performed.
Still, they are not mandatory in every encounter. A rushed, superficial abstraction test can add little value if the presenting issue is acute agitation or suicidal crisis. This is where structured documentation helps – it reminds clinicians what to consider while allowing adaptation to the actual clinical situation.
Insight, judgment, and reliability
Insight refers to the patients awareness and understanding of their condition, symptoms, or need for treatment. Judgment reflects decision-making capacity in real-world situations. These are often documented together, but they should not be treated as identical.
A patient can have limited insight into illness yet show intact judgment in some domains. Another may acknowledge severe symptoms but continue making dangerous choices. Reliability is also worth noting when the history appears inconsistent, limited by psychosis, impaired memory, intoxication, or guardedness.
These sections matter because they affect everything downstream, including discharge planning, adherence, collateral needs, and whether the patient can participate meaningfully in treatment decisions.
Risk assessment is often part of a complete MSE
Strictly speaking, some clinicians document suicide and violence risk outside the MSE in a separate risk section. Operationally, though, risk-related findings are often embedded in thought content, perception, judgment, and behavior. For that reason, many clinicians reasonably think of risk assessment as part of a complete mental status evaluation.
What matters most is not where it sits in the note, but whether it is clearly addressed. If a patient endorses suicidal ideation, the documentation should move beyond yes or no. Intent, plan, means, recent behavior, protective factors, and level of immediacy all shape clinical significance. The same applies to homicidal ideation, aggression risk, grave disability, and vulnerability due to impaired cognition or psychosis.
What changes by setting?
The components stay broadly consistent, but emphasis shifts. In emergency psychiatry, clinicians usually prioritize agitation, psychosis, intoxication, orientation, and immediate safety. In consultation-liaison settings, cognition, attention, fluctuation, and medical contributors may deserve more space. In outpatient therapy or psychiatry, the MSE may be briefer but still needs to capture mood, affect, thought process, perception when relevant, and functional judgment.
This is also where templates are most useful. A standardized framework reduces the risk of missing core domains while still allowing setting-specific detail. On MentalStatusExamTemplate.com, that practical balance between consistency and flexibility is exactly what makes documentation faster without making it generic.
Common documentation mistakes
The most common problem is overcompression. Notes that say “AAOx3, mood okay, affect appropriate, thought process normal” may save time in the moment, but they often fail to support the complexity of the visit. Another issue is mixing observation with interpretation too quickly. “Manipulative” is less useful than describing the behavior that led to that impression.
It is also easy to document contradictions without clarifying them. If the patient denies hallucinations but appears distracted and responds to unseen stimuli, both pieces belong in the note. The MSE should reflect the clinical reality, including uncertainty.
A good mental status exam is complete enough to communicate clearly, selective enough to stay relevant, and objective enough to hold up under review. When clinicians use a consistent structure, they chart faster, miss less, and give the next provider something they can actually use.



2 Comments