Psychiatric Intake MSE Example That Works

A psychiatric intake MSE example is most useful when it reads like documentation you could actually place in a chart, not a textbook exercise. At intake, clinicians are balancing rapport, safety, diagnostic clarity, and time pressure. The mental status exam has to capture the patient’s current presentation accurately enough to guide treatment and support handoff, while staying concise enough to be usable.
That is where many notes break down. They become either too sparse to support clinical reasoning or so bloated with generic phrases that they stop communicating anything meaningful. A strong intake MSE does not try to say everything. It documents the observations and patient-reported features that matter for this encounter, this level of care, and this risk profile.
What a psychiatric intake MSE example should show
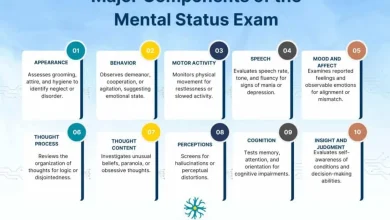
At intake, the MSE is not just a checklist. It is a structured snapshot of the patient’s functioning at the time of evaluation. In practice, that means the note should reflect observed behavior, speech, affective presentation, thought process, thought content, cognition as assessed, and judgment and insight, all documented in language specific enough to be defensible.
A good example also avoids false precision. If cognition was not formally tested beyond orientation and conversational attention, the note should not imply a full neurocognitive exam. If insight is partial, say partial. If affect is constricted but reactive, document both. This level of specificity improves clinical communication and reduces the risk of copy-forward charting that no longer matches the patient in front of you.
Psychiatric intake MSE example
Below is a realistic sample for an adult outpatient psychiatric intake:
Appearance: Adult female, appears stated age, casually dressed, grooming adequate, hygiene intact. No acute distress.
Behavior: Calm, cooperative, engaged in interview. Maintains appropriate eye contact. No psychomotor agitation or retardation noted. No abnormal movements observed.
Speech: Normal rate, rhythm, and volume. Speech coherent and spontaneous.
Mood: “Overwhelmed and down.”
Affect: Constricted but congruent with stated mood. Appropriate to discussion content.
Thought process: Linear, logical, and goal-directed.
Thought content: Denies current suicidal ideation, homicidal ideation, delusions, or paranoia. Reports excessive guilt and rumination related to work and family stressors. No obsessions elicited.
Perception: Denies auditory or visual hallucinations. No evidence of responding to internal stimuli.
Cognition: Alert and fully oriented to person, place, time, and situation. Attention grossly intact throughout interview. Recent and remote memory grossly intact by conversational testing.
Insight: Fair. Acknowledges depressive symptoms and need for treatment.
Judgment: Fair. Seeking care voluntarily and able to discuss treatment options appropriately.
This works because it is clear, restrained, and specific to the encounter. It gives another clinician a usable picture of the patient without overstating certainty.
Why this psychiatric intake MSE example works clinically
The value of this psychiatric intake MSE example is not in the wording alone. It works because each section contributes something clinically relevant. Appearance and behavior establish observable baseline functioning. Speech, mood, and affect help characterize current emotional and psychiatric state. Thought process and thought content help distinguish distress from disorganization, psychosis, or acute risk. Cognition, insight, and judgment support both diagnostic formulation and treatment planning.
Just as important, the note separates what was observed from what was reported. Mood is patient-reported. Affect is clinician-observed. Hallucinations may be denied, but responding to internal stimuli is an observation. That distinction matters in both clinical and legal-quality documentation.
How to adapt the example to different intake settings
The same MSE framework applies across settings, but the emphasis changes.
In the emergency department, your note may need tighter language around agitation, intoxication, orientation, and immediate safety risk. A patient in crisis may not permit a lengthy cognitive assessment, so your documentation should reflect what was actually assessable. For example, attention may be impaired by internal preoccupation, severe anxiety, or substance use. That is more useful than defaulting to “grossly intact” when it clearly was not.
In an inpatient psychiatric admission, the MSE often needs more detail about psychosis, behavioral control, and functional impairment. If the patient is guarded, internally preoccupied, or disorganized, that should appear in behavior, thought process, and perception. Intake notes in this setting also benefit from documenting whether reliability as a historian is limited.
In outpatient psychiatry or therapy intake, the MSE may appear more stable, but it should still be specific. Clinicians sometimes under-document thought content or judgment when the patient is pleasant and organized. That can leave gaps, especially if depressive symptoms, trauma symptoms, or passive death wishes emerge later in the interview.
Common charting mistakes to avoid
The most frequent problem is generic documentation. Phrases like “within normal limits” or “normal” are quick, but they often communicate very little. Normal compared to what? In psychiatric charting, descriptive language is usually stronger than broad labels.
Another mistake is internal inconsistency. A note that describes the patient as highly distracted and tangential should not also list attention as intact and thought process as linear unless there is a clear explanation. Review the MSE as a whole before signing it. The sections should align with one another and with the HPI.
Over-documentation can also create risk. If you auto-populate a full cognitive section, but only assessed orientation and conversational memory, the record becomes less reliable. Complete documentation is not the same as inflated documentation.
There is also the issue of vague affect terms. “Appropriate” by itself is often too thin. Appropriate, but how? Full range, constricted, blunted, tearful, labile, reactive, mood-congruent – these add clinical value and support better continuity between providers.
A practical framework for writing your own intake MSE
When time is limited, it helps to think in sequence: what the patient looks like, how the patient engages, how the patient speaks, what the patient reports feeling, what you observe emotionally, how the patient thinks, what the patient is thinking about, whether perception is altered, what cognitive functions were assessable, and how insight and judgment appear today.
That sequence keeps the note organized and reduces omissions. It also helps newer clinicians avoid jumping straight to diagnostic interpretations. The MSE should describe current mental functioning first. Your formulation can then explain what those findings may mean.
In many workflows, standardization is what improves quality most. A repeatable structure lowers cognitive load and makes it easier to notice meaningful abnormalities. That is one reason clinicians often rely on a consistent template rather than composing every note from scratch. MentalStatusExamTemplate.com focuses on exactly this problem: helping providers standardize MSE documentation without losing clinical specificity.
Example variations based on presentation
If the patient is manic, the same structure remains useful, but the content changes substantially. Speech may be pressured, affect expansive, thought process circumstantial or flighty, judgment impaired, and insight limited. If the patient is severely depressed, psychomotor slowing, reduced eye contact, soft speech, and impoverished thought content may become central features.
For psychosis, precision matters even more. Instead of writing “psychotic,” document the observed and reported findings: guarded behavior, thought blocking, persecutory delusions, auditory hallucinations, loose associations, or poor reality testing. The note becomes stronger when it shows the basis for the impression.
For trauma-related or highly anxious presentations, thought process may remain linear while attention is impaired by hyperarousal. Affect may be constricted, tearful, or anxious but still reactive. That nuance matters because not all distressed patients show formal thought disorder, and not all concentration problems indicate primary cognitive impairment.
Documentation tips that improve accuracy fast
Use quoted language selectively when it sharpens the clinical picture, especially for mood, delusional content, or risk-related statements. Keep the rest of the MSE in plain, professional prose. Avoid mixing interpretive labels into observational sections unless the finding is well supported.
If something could not be assessed, say that. If the patient was too sedated, too guarded, or too disorganized for a full evaluation, document the limitation directly. That is better documentation than filling gaps with default wording.
It also helps to read the MSE alongside your assessment and plan. If your plan reflects high acute risk, severe disorganization, or inability to care for self, the MSE should contain findings that support that level of concern. Good documentation is not just complete section by section. It is coherent across the note.
A strong intake MSE does not need to be long to be clinically useful. It needs to be accurate, internally consistent, and tailored to what you actually observed. If your note helps the next clinician understand the patient’s presentation within a few seconds of reading it, you are doing the job well.