What Is MSE Mental Status Examination?

If you have ever asked, “what is MSE mental status examination,” you are usually not looking for a textbook definition alone. You are trying to understand what belongs in the exam, how it guides clinical judgment, and what needs to be documented clearly enough to support diagnosis, handoff, and treatment planning.
The mental status examination, or MSE, is a structured clinical assessment of a patient’s current psychological functioning at the time of the encounter. It captures what the clinician observes directly and what the patient reports during the interview. In practice, it serves as the behavioral health equivalent of a physical exam. It does not replace history, collateral information, labs, or formal cognitive testing, but it gives a real-time snapshot of the patient’s mental condition that can immediately affect risk assessment and disposition.
What is MSE mental status examination used for?
The MSE is used to organize clinical observations into a consistent framework. That structure helps clinicians identify abnormalities, compare findings over time, and communicate clearly with other providers. In inpatient psychiatry, it may support admission decisions or daily progress notes. In the emergency department, it can clarify whether agitation, disorganization, or altered behavior suggests intoxication, delirium, psychosis, mania, or severe mood disturbance. In outpatient care, it helps track symptom severity, functional change, and treatment response.
A well-documented MSE also reduces a common charting problem: vague language. Phrases like “doing better” or “appears off” do not tell the next provider what was actually observed. By contrast, documenting that speech was pressured, affect was constricted, thought process was tangential, and insight was limited creates a much more usable clinical picture.
The core components of an MSE
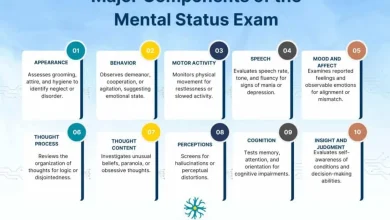
Although exact formatting varies by setting, most mental status exams cover the same domains. The value is not in memorizing labels. The value is in assessing each domain deliberately and documenting what is clinically relevant.
Appearance and behavior
This section describes what is immediately observable. It may include grooming, hygiene, dress, eye contact, posture, psychomotor activity, gait, level of cooperation, and overall engagement. A patient may appear disheveled, guarded, restless, withdrawn, or appropriately dressed for weather and setting.
Behavioral observations matter because they often provide the earliest clues to psychiatric or medical instability. Psychomotor retardation may support severe depression. Marked agitation may raise concern for intoxication, mania, psychosis, or escalating risk.
Speech
Speech is often documented by rate, volume, quantity, fluency, and tone. It may be normal, slowed, pressured, loud, soft, sparse, monotone, or hesitant. The point is to describe how the patient communicates, not just whether they are talkative.
Speech abnormalities can narrow the differential quickly. Pressured speech may suggest mania. Long latency or impoverished speech may occur in depression, psychosis, neurocognitive disorder, or negative symptoms.
Mood and affect
Mood is the patient’s stated emotional experience. Affect is the clinician’s observation of emotional expression. These are related but not interchangeable. A patient may report feeling “fine” while presenting with tearful, constricted affect, or report anxiety with visibly tense, reactive affect.
Good documentation often addresses quality, range, intensity, and congruence. For example, affect may be flat, blunted, constricted, full range, labile, or congruent with stated mood. This distinction improves precision and prevents the common mistake of documenting mood and affect as if they were the same finding.
Thought process
Thought process describes how ideas are connected and expressed. Clinicians often assess whether thinking is linear, goal-directed, circumstantial, tangential, loose, disorganized, or perseverative. This is one of the most important sections for distinguishing organized distress from formal thought disorder.
A patient can have intense symptoms but still demonstrate coherent thought process. Another patient may say very little that is overtly bizarre, yet show severe disorganization through derailment and loose associations.
Thought content
Thought content refers to what the patient is thinking about. This may include delusions, obsessions, preoccupations, phobias, ruminations, ideas of reference, suicidal ideation, homicidal ideation, hopelessness, guilt, or violent thoughts.
This domain is clinically sensitive and often risk-critical. It should be documented with specificity when relevant. “Denies SI/HI” is common shorthand, but in many encounters it is better to document whether ideation, plan, intent, means, and protective factors were assessed.
Perception
Perceptual disturbances include hallucinations, illusions, depersonalization, and derealization. If hallucinations are present, documentation should ideally clarify modality, frequency, intensity, and impact. Auditory hallucinations are not the same as command hallucinations, and both differ from trauma-related intrusive experiences.
This is one area where overgeneralization creates avoidable confusion. A brief note that the patient is “psychotic” is less useful than specifying that they report persecutory delusions and intermittent auditory hallucinations without command content.
Cognition
Cognition in the MSE usually includes orientation, attention, concentration, memory, and sometimes fund of knowledge or abstract reasoning. The depth of assessment depends on the setting. In an emergency department, a focused screen may be enough. In outpatient neuropsychiatric work, a more detailed cognitive assessment may be needed.
This section is especially important when delirium, intoxication, withdrawal, traumatic brain injury, dementia, developmental disorder, or severe psychosis is in the differential. Cognitive findings may significantly affect capacity, reliability, and disposition.
Insight and judgment
Insight refers to the patient’s awareness and understanding of their condition. Judgment reflects decision-making capacity in practical situations. These findings are often documented briefly, but they should not be treated as filler.
Limited insight may affect adherence, safety planning, and treatment engagement. Impaired judgment may show up in recent dangerous behavior, inability to recognize consequences, or poor decision-making related to substance use, self-care, or aggression.
What the MSE is not
A mental status exam is not the same as a psychiatric history, a full diagnostic evaluation, or a standardized rating scale. It is one component of assessment. That distinction matters because clinicians sometimes overstate what the MSE can establish on its own.
For example, an MSE can show that a patient is inattentive, disoriented, paranoid, or internally preoccupied. It cannot by itself determine whether the cause is schizophrenia, stimulant intoxication, delirium, trauma, or a neurological condition. The exam supports clinical reasoning, but it does not replace it.
How clinicians actually use the MSE in practice
In real settings, the MSE works best as both an assessment tool and a documentation framework. During the encounter, it keeps the clinician from skipping key domains. After the encounter, it helps convert observations into chart language another provider can use.
That is where standardization becomes practical rather than bureaucratic. A repeatable MSE format reduces omissions when the unit is busy, the patient is complex, or the presentation is evolving. It also improves comparisons across time. If one note says “anxious” and the next says “better,” that tells you very little. If the later note shows improved eye contact, normal speech rate, reduced psychomotor agitation, linear thought process, and denial of current suicidal ideation, the clinical change is much clearer.
Common documentation mistakes
The most frequent problem is vagueness. The second is contradiction. A note may describe a patient as calm and cooperative, then later document severe agitation without explaining the change. Another common issue is using diagnostic labels in place of observations, such as writing “manic” instead of describing elevated mood, decreased need for sleep, pressured speech, and flight of ideas.
There is also a trade-off between speed and precision. In high-volume settings, clinicians need efficiency. But over-shortened charting can become legally weak and clinically unhelpful. Using a structured template can help preserve completeness without slowing workflow. MentalStatusExamTemplate.com is built around that exact need.
What is MSE mental status examination in different settings?
The answer depends somewhat on where you practice. The core domains stay stable, but emphasis changes by environment.
In the emergency department, the MSE often prioritizes safety, orientation, agitation level, psychosis, intoxication, and immediate risk. In outpatient therapy, mood, affect, thought content, insight, and functional change may take center stage. On a medical floor, cognitive findings may matter more because delirium and medical causes of behavioral change have to stay high on the list.
That is why one-size-fits-all wording can be a problem. The best MSE format is standardized enough to prevent omissions and flexible enough to match the clinical setting.
Why this exam still matters
The MSE remains central because it turns subjective interaction into organized clinical data. It sharpens observation, supports risk assessment, improves interdisciplinary communication, and creates a defensible record of the patient’s presentation at a specific moment in time.
For trainees, it teaches how to notice what matters. For experienced clinicians, it prevents drift into shorthand that loses meaning. And for any team managing psychiatric or behavioral presentations under time pressure, a clear MSE often makes the difference between a note that is merely completed and one that is actually useful.
The most helpful approach is to treat the MSE less like a form to finish and more like a disciplined habit of observation – one that makes your assessment clearer, your documentation stronger, and your next clinical decision easier to defend.



2 Comments